Boutonniére Deformity
Description
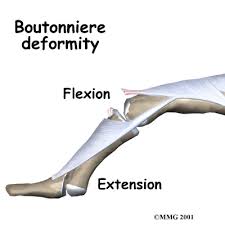
Boutonnière Deformity, which is French for Buttonhole Deformity, is a weakness and loss of extension of the PIP joint, in addition to hyperextension and decreased active and passive flexion of the DIP joint. The central tendon is disrupted when there is sudden forced flexion of the actively extended PIP joint. The lateral bands of the extensor expansion dislocate volar to the PIP joint axis, which limits motion in this joint. This limitation leads to contractures of the oblique retinacular ligament, volar plate of PIP joint, and collateral ligaments of DIP joint.
Signs & Symptoms
Five stages of Boutonnière Deformity:
Stage 1
|
|
Diagnostic Tests
- Elson Test: Evaluate the integrity of central slip by positioning PIP in 90 degrees of flexion and comparing the resting position of the DIP joint with the uninvolved digit. The patient is then asked to actively extend involved PIP joint against resistance (disruption of central tendon would show weakness). DIP joint would also be hyperextended and passive flexion restricted.
- Boyes Test: Active flexion of DIP joint is limited when PIP joint is passively positioned in full extension.
PT Implications
Treatment depends on stage of healing:
- Acute (within 2 weeks)- immobilization of PIP joint in full extension for 4 to 5 weeks with static splint that allows active and passive DIP flexion
- Subacute (2-8 weeks)- when PIP can be passively extended, extension splinting is treatment of choice. Flexion contractures of PIP that are not yet fixed may respond to dynamic and/or static progressive extension splinting to avoid surgery.
- Chronic (more than 8 weeks)- difficult to address with splinting so anatomic repair of central slip and lateral bands is recommended. If arthritis pain from degeneration, arthrodesis can be effective.
